I searched and searched for a diagnostic approach that would give me answers, and finally, one very lucky day, I found it!
A group of Canadian researchers produced a study that led to them developing the Gross Motor Function Score Classification System or GMFSC for short. This study is the most reputable of all studies and has been validated in many other countries and upheld as true. As I discovered, medical people in the CP research industry know all about it and currently they are debating whether the scoring for milder CP could be done more specifically. But most importantly, on the whole this is where one finally gets to stare at the truth your child’s gross motor future.
Put very simply, this is a score sheet called the GMFM-66. This sheet allows you or your therapist to add up your child’s gross motor abilities. The total score gets calculated as a percentage. The researchers followed a very large group of children between the ages of 2 and 18 (in various studies and since repeated in various countries) over time. Only children who had had botulinum injections and surgery were excluded in the final analysis because they wanted to see how the development takes place without such interventions.The study looked at kids who got many therapies five days a week, to those who did less, and even included those children who did not get any therapy at all.
From this they saw that when you plot the data, it forms clusters (dots close together) and from these clusters they could plot five development curves over time. This can get really complicated, so I will only give the broad strokes for children between two and six:
Prognosis for Gross Motor Function in Cerebral Palsy: Motor Development Curves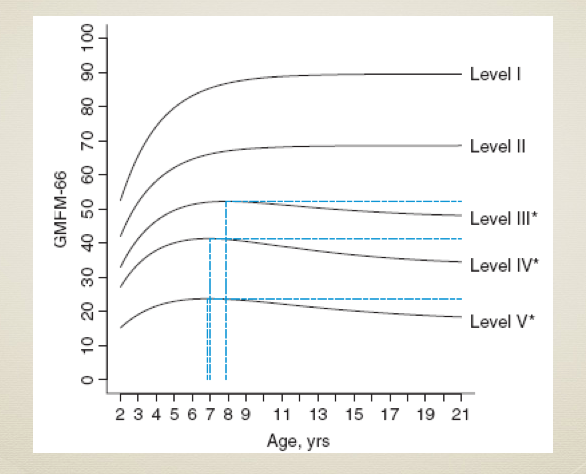
Peter L. Rosenbaum; Stephen D. Walter; Steven E. Hanna; et al. JAMA. 2002;288(11):1357-1363
Level 1 represents children who walk by the age of two but are a little clumsy.
Level 2 are children who walk late. Before the age of four they often use a walker and the learn to walk freely by the time they are four.
Level 3 are the ones who can sit and crawl a bit. They use a walker indoors but will need a wheelchair in the community.
Level 4 represents kids who have some head control and can sit with some support. They can maybe roll and possibly do bunny-hop crawling. They could learn to use a walker later but will mostly use wheelchairs.
Level 5 are those kids who cannot move against gravity, battle with head control and who needs high trunk support to sit. Kids on level 4 and 5 will use a wheelchair and, if arm function permits it, can be self-steered with a joy stick or eye control.
These curves are tight and do not typically change despite numerous therapies. This means that by the time you are able to plot a child on a level or curve (2.5 years to 3.5 years) this is where they tend to stay.
Sadly, children who do not walk (levels 3-5) reach a peak between 6 and 8 years (degree of therapy notwithstanding) and then the researchers found that they deteriorated!
The only thing that can possibly change this is therapy/treatment that can change the actual structure of the child. Here I have established the following list:
You can choose to try botulinum toxin, but clinical evidence quite clear that repeated botulinum injections do not prevent structural deterioration and while there may be short-term (weeks/months) apparent “improvements”, the price one pays is loss of muscle function and micro scarring (fibrosis) of the muscle.
Surgeries, such as SPML surgery and the more invasive kinds of releases again can change structure that would give localised release, but it is debatable how long these changes last and how soon the surgery needs to be repeated. This is what the evidence suggests. Surgery also cannot improve head or trunk control. To be able to walk or stand, one needs head and trunk control.
There’s a third option, one that doesn’t require injections or surgery. It is the route we chose. We started with a home-based therapy known as ABR (Advanced Biomechanical Rehabilitation) because it can change structure in a global fashion. Recent research has found that ABR improves quality of life in children with severe CP, gives neck and trunk control with the significantly improved ability to sit. Indeed, by the end of this study, children who started as GMFSC level 5 had scores that put them on GMFSC level 4, But this is another topic I will discuss later.
Emma fell just below the curve for level 4 CP, so head control and trunk control were real issues for us. This made the choice to do ABR very clear.

One thought on “A real Answer? My Child’s Gross motor future.”