
Like many children with Cerebral Palsy, Emma has always struggled with sleep. Here’s my approach to ensure she (and me) has the best possible chance of rest.
One of the reasons I don’t post on this blog as regularly as I would like is because I live my life in the twilight zone of fatigue. This is because ever since she was born, Emma has been a poor sleeper. In fact, she didn’t even sleep during the day- this meant we never had the rest we needed.
I have been on a mission to work out a sensible approach to help her, but I have yet to find the magic solution. What I can say is that we have greatly improved her sleep pattern – but it’s been very hard work.
Sleep is a complex issue in Cerebral Palsy. One out of five kids with CP has issues with sleep, and the more severe the CP, the more likely he/she is to have issues with sleep.
There are many reasons why children with CP don’t sleep well. Some issues have been described and studied, but the literature agrees that it’s not completely understood.
My approach to Emma’s lack of sleep has taught me a thing or two, I hope this will help you and your child.
Kids with severe CP have a common sleep disturbance called Sleep Disordered Breathing (SDB) . This can be broken down into three sub-themes.
- Obstructive Sleep Apnoea: this is where the upper airway is obstructed and even though the child is breathing, air cannot flow properly into the lungs. It could be due to poor muscle tone, palate deformities or even something like large tonsils blocking the airway.
- Central Sleep Apnoea: Is a central problem that interferes with breathing. What I mean with central is that the brain centre that controlls breathing isn’t functioning correctly. In other words, a “computer” problem rather than a mechanical problem. This is very common in people who have had some kind of brain injury.
- Mixed: this is where both of these issues are present.
In children the obstructive type is most common. And, of course, there are other issues that can interfere with sleep. For example, kids with epilepsy can have poor quality sleep, are often tired during the day and may grind their teeth while asleep. In addition, pain or reflux could also be an issue.
But there are other issues, too. When Emma was struggling badly a few years ago, I took her to an ear, nose and throat specialist who said that she might have an allergy that was causing her nose to block. I was told to try a nose drop and report back to him.
The nose drop made no difference. I realised that I was going to have to work this out on my own. I noticed that Emma was very anxious at night when going to bed. She struggled to fall asleep and struggled to stay relaxed while sleeping. Often she would wake up with a start.
One day I was watching a video that Leonid Blyum (the founder of ABR) had shared with me. In it he spoke about emotional fear leading to physical tension and fear, and that kids with severe CP cannot get rid of this inner tension the way a healthy person can. There is no way for them to stretch, scream, laugh out loud or change their pattern of breathing. They have no way to release their inner tension.
He said something that still makes me pause. He said that the child with GMFSC 5 severe CP is functionally just a head with no body because there is no body map available in that brain. This leads to these children experiencing extreme anxiety because nothing in their experience and movement world makes any sense. He talked about this being like a type physiological “decapitation”. An extreme idea, but boy that gave me insight into the kinds of fear Emma must be feeling every day!
She must have, especially in the beginning, felt that she was in constant free fall.
Looking at her spontaneously going into a Moro reflex (where a baby spreads out its arms, then contracts them and cries, in response to the idea they’re falling) while lying safely on the ground, was evidence enough for me. The simple act of moving her into a different position was, judging by her reaction, like an earthquake to her.
I knew that my sleep strategy for her needed to be adjusted. I had to work on her deep sensory sensation with a deep and firm touch, to activate those nerve bodies that lay in the deeper tissue layers. This would give her body a sense of “hold” and just may help her to relax while she tries falling asleep. This is, after all, what we do with babies, we swaddle them in a firm wrap.
It’s not a new concept, in fact there are some assistive devices that can help when a child is like this. For example, a weighted blanket, or wearing a posture support suit, such as a Theratog, would achieve the same thing.
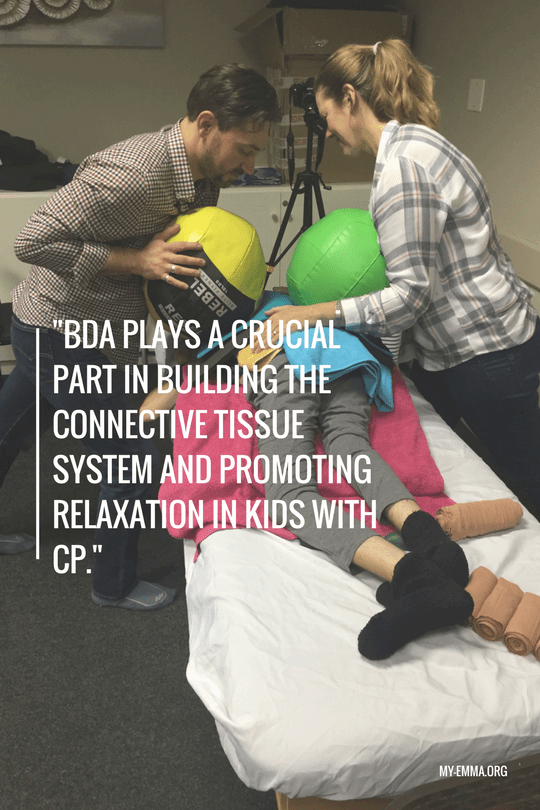
I also realised that I needed to continue with connective-tissue-based therapy. This plays a crucial part in building the connective tissue system and promoting relaxation in kids with CP.
In our case, we do BDA. This therapy takes time and needs to be done every day, but if you do it, your child will develop a body map. Through mechanical stimulation, the dysfunctional connective tissue of CP will remodel into healthier, stronger and more flexible tissue. Better connections will form. When we examine children with CP, it is very clear that the connective tissue links between skin and muscle, muscle and muscle, muscle and bone are disturbed. No wonder these children don’t know or feel their bodies, because the information from the tissue to the brain will be very distorted when such “disconnection” is present. With connective-tissue-based therapy, these underdeveloped connections start to develop, proprioception (the ability to know where your body is in space) develops and in so doing, the brain gets better data from the system and a better body map can form.
This is not the only place where BDA can help sleep. It can also help by shaping body cavities that hold and don’t collapse. Kids with CP often have abnormal breathing patterns and chest and spine deformities. BDA can go very far to help or, in some cases, even fix these issues. Deeper, more regular breathing means better sleep.
The following before and after images have been provided by BDA to illustrate the point I am making:
 So here is an approach to help your child’s sleep:
So here is an approach to help your child’s sleep:
- First, exclude the issue of potential upper airway obstruction, such as tonsils or adenoids etc. I did this by visiting an ear, nose and throat specialist.
- Then exclude the issue of reflux (by referring to your paediatrician or ear nose and throat specialist).
- Make sure epilepsy is controlled. You might need a sleep EEG for that. If your child tends towards epilepsy, I would consider doing a hair analysis for metals, nutrients and amino acids balances. This can be done by visiting an integrative practitioner or naturopath. I would also consider using medical cannabis if the epilepsy isn’t controlled.
- Work on their nutrition (see my previous posts for this).
- Do a connective-tissue-based therapy. In our case, it’s BDA, but as you know ABR is also recommended.
- If you think there is a sensory issue, try using a weighted blanket or tuck a light sheet firmly over your child while sleeping. Help them to release inner tension by doing physical activity such as swimming and avoiding overstimulation and blue light before bed. Follow a regular bed-time routine.
-
Make sure your child drinks enough fluid during the day and if your child wakes, ask if they’re thirsty. Due to open-mouth breathing and drooling – combined with tissue that tends to be dehydrated – your child might not be able to fast through an eight-hour night. Keep some flavoured water or diluted juice nearby and offer it to them. (If find Emma swallows flavoured drinks better than neutral tasting drinks but this may not be a factor for everyone.)
- Avoid constipation. Use stool softeners such as Movicol or even paediatric enemas. A blocked stomach will definitely interfere with sleep.
- A good nose drop will help with disrupted sleep during an upper airway infection.
- The following natural supplements have been of value to us:
Melatonin 3mg (will help with falling asleep).
Melatonin Slow Release (eg. Circadin) helps a person to fall asleep and stay asleep.
Passionflower syrup can help induce drowsiness.
Magnesium, especially, if your child tends towards sensory problems, spasticity and epilepsy.
I hope my experience with Emma goes some way to help you find a better sleeping pattern for your child. Let me know how it goes.
